Periodontal disease is defined as a plaque-induced pathology of the periodontium (the supporting structures of the tooth) and ranges from gingivitis (stage I) to varying degrees of attachment loss (stages II-IV). There are many forms and causes of this disease and early detection, diagnosis and treatment are essential for desirable outcomes. This case report presents the successful treatment of a three-walled infrabony defect of a left maxillary canine tooth in a dog through open root planing, bone graft & barrier membrane placement, and coverage by healthy gingiva.
A 7-year-old, 10.5 kg male neutered Dachshund was presented for oral examination by the owners for halitosis. No other concerns were expressed and pre-examination history conveyed by the owners were consistent with that of a healthy canine. Gross oral examination showed severe calculus with moderate to severe gingivitis. The reported halitosis was also observed. No dental procedures had been performed to date and the canine had no previous history of any major health problems.
There are various treatment options for periodontal disease and the chosen treatment should take into consideration a number of factors including the type of disease present, the extent, the distribution, and the severity. Since grades 2, 3, and 4 occur subgingival, intraoral radiographs and oral examination with periodontal probing under general anesthesia are required to correctly diagnose and treat patients with periodontal disease.
Treatment options for the various stages of periodontal disease were discussed with the owners. A plan was made for the canine patient to return for a comprehensive oral health assessment & treatment with full mouth intraoral radiographs under general anesthesia.
Treatment
Full mouth intraoral radiographs were obtained, under general anesthesia, revealing approximately 35-40% vertical bone loss associated with tooth 204. Other teeth with disease were noted but will not be discussed here.
Periodontal probing and exploration also revealed 7mm infrabony pocketing along the palatal aspects of tooth 204. Intraoral radiographic and oral examination findings were consistent with stage III periodontal disease (greater than 25% but less than 50% bone loss).
A left infraorbital nerve block was placed with 0.5% bupivacaine solution. A full thickness mucogingival flap was created and elevated buccally. The palatal tissue was then elevated exposing a 3-walled periodontal pocket along the palatal aspect of tooth 204.
Meticulous cleaning and smoothing of the pocket and root surface was performed manually using various curettes. Bone allograft was then placed into the 3-walled pocket and a biological membrane was placed over the bone graft. The full thickness flaps were then sutured into their original positions using 4-0 monofilament synthetic absorbable suture.
Follow-up
The 4 week recheck showed the gingiva over the treatment site to be intact without evidence of inflammation, dehiscence or trauma.
The patient was readmitted 12 months after treatment where a follow-up oral examination and intraoral radiograph of tooth 204 were performed. The gingiva covering the periodontal treatment site of tooth 204 appeared pink, intact, and non-edematous. An intraoral radiograph of tooth 204 was obtained demonstrating healing of the infrabony pocket with regeneration of alveolar bone, periodontal ligament, and lamina dura. This indicated that appropriate osteogenesis and reattachment of the periodontal apparatus had occurred.

Pre-operative intraoral photograph.
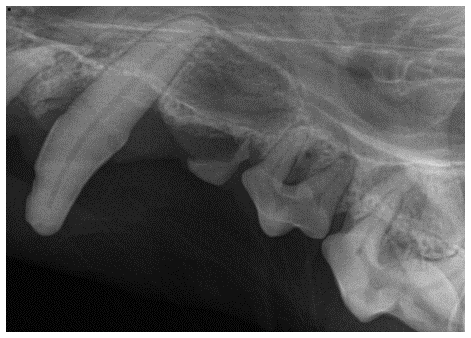
Pre-operative radiograph of tooth 204 showing stage III periodontal disease. Pathology with other teeth is noted but not discussed here.
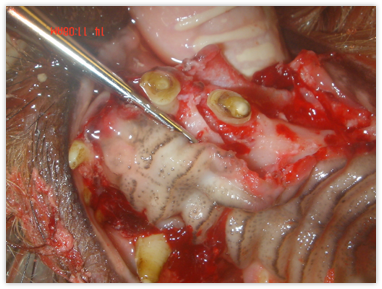
Elevation of mucogingival and palatal flaps showing a 3-wall infrabony pocket along the palatal aspect of tooth 204.

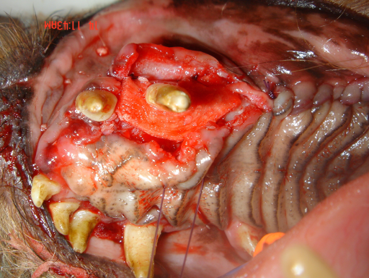
Placement of biologic membrane over the infrabony pocket after root planing and bone graft placement.

Treatment site after closure of mucogingival and palatal flaps.

Gingival healing 4 weeks post-op.

Intraoral radiograph taken 1-year post-op showing osseous and periodontal regeneration.
Case submitted by: Kevin Haggerty, MVB, DAVDC